
Your Knee Pain Isn't a Knee Problem: The Hidden Foot-Hip Connection
Your Knee Pain Isn't a Knee Problem: The Hidden Foot-Hip Connection
In my last blog, we talked about arch collapse and how problems at your feet don't stay at your feet. Today, I want to dive deeper into something I see almost daily in practice: patients suffering with chronic knee and hip pain who've tried everything—physical therapy, injections, medications, even surgery, but nothing provides lasting relief.
Here's why: they're treating the knee and hip, but ignoring what's causing the problem in the first place.
Your knees and hips are caught in the middle of a biomechanical tug-of-war. Below them, your feet are (often) collapsing and rotating inward. Above them, your pelvis and spine are trying to stay upright and balanced. And right in the middle? Your knees and hips are forced to twist, compensate, and absorb stress they were never designed to handle.
Let me show you exactly what's happening in your body—and more importantly, how to fix it at the source instead of just chasing symptoms.
The Knee: Your Body's Most Vulnerable Joint
Your knee is basically a hinge joint; it's designed to bend and straighten in one plane of motion. Unlike your hip (which is a ball-and-socket joint that moves in multiple directions) or your ankle (which can tilt and rotate), your knee has very limited ability to handle rotation or side-to-side stress.
This makes it incredibly efficient for walking and running when everything is aligned properly. But it also makes it extremely vulnerable when forces from above or below push it out of its ideal position.
Think of your knee like a door hinge. When the door frame is straight and level, the hinge works smoothly for decades. But if the frame tilts or twists, that hinge starts grinding, binding, and eventually breaks down no matter how strong the hinge itself is.
That's exactly what happens when your feet collapse.
What Collapsed Arches Do to Your Knees
When your arches flatten and your feet roll inward (overpronation), here's the mechanical nightmare that unfolds at your knee:
The Rotation Problem
Your shinbone (tibia) rotates internally
- As your foot pronates, it forces your tibia to twist inward
- This rotation happens with every single step you take
- Over thousands of steps per day, this repetitive rotation creates massive stress
Your kneecap (patella) tracks improperly
- The patella is supposed to glide smoothly in a groove at the end of your thigh bone
- When your tibia rotates inward, it pulls the patella off-center
- The kneecap now grinds against the side of the groove instead of gliding smoothly
- This is called patellofemoral pain syndrome—one of the most common knee problems
The Stress Distribution Problem
Normal knee mechanics distribute force evenly across the joint. But when your foot collapses:
The inner (medial) knee gets overloaded
- Your body weight shifts to the inside of your knee
- The medial meniscus (cartilage shock absorber) gets compressed excessively
- The medial collateral ligament (MCL) gets overstretched
- Bone-on-bone contact increases on the inner knee
The outer (lateral) structures get pulled tight
- Your IT band (iliotibial band) becomes taut and irritated
- The lateral meniscus experiences abnormal shearing forces
- Tension builds up on the outside of your knee
The result: You develop pain that feels like it's coming from your knee, because it IS hurting there, but the root cause is 12-18 inches below at your foot.
Common Knee Conditions Caused by Foot Problems
- Patellofemoral pain syndrome (runner's knee)
- IT band syndrome (lateral knee pain)
- Medial knee osteoarthritis (inner knee degeneration)
- Patellar tendonitis (jumper's knee)
- Meniscus tears (particularly medial meniscus)
- ACL injuries (the twisting mechanism increases risk)
One study found that people with flat feet were significantly more likely to develop knee pain and osteoarthritis compared to those with normal arches. Another showed that correcting foot pronation with orthotics reduced knee pain by an average of 43% in just 12 weeks.
Real Patient Story: The Runner Who Couldn't Run
Meet Tom, a 38-year-old runner who came to see me after developing severe knee pain. He'd been running for years without problems, but over the past six months, his right knee started hurting so badly he had to stop running completely.
He'd already seen an orthopedic surgeon who diagnosed him with patellofemoral pain syndrome and recommended physical therapy. Tom did 12 weeks of PT: quad strengthening, stretching, foam rolling. It helped a little, but as soon as he tried to run again, the pain came roaring back.
When I evaluated Tom, here's what I found:
At his feet:
- Moderate overpronation, worse on the right
- Collapsed medial arch
- His right shoe showed significant wear on the inside edge
At his knee:
- Right tibia rotated internally, more than the left
- Kneecap tracking laterally (to the outside)
- Pain with patellar compression
- Tight IT band on the right
At his hip and pelvis:
- Right hip internally rotated
- Pelvis rotated to compensate
- Weak right glute muscles
Tom's knee wasn't the problem; it was the victim of what was happening below and above it.
Our treatment plan:
- Chiropractic adjustments to restore proper mechanics in his foot, ankle, knee, and hip
- Custom orthotics to control his overpronation and support his arches
- Specific exercises to strengthen his glutes and improve hip stability
- Gradual return-to-running protocol
Within 8 weeks, Tom was running pain-free. We didn't "fix" his knee, we removed the forces that were destroying it.
The Hip: Where Foot Problems Meet Spine Problems
If knees are vulnerable because they're hinge joints, hips are vulnerable because they're the connection point between your lower body and your spine. When your feet collapse, the stress doesn't stop at your knees, it continues upward to your hips.
What Foot Collapse Does to Your Hips
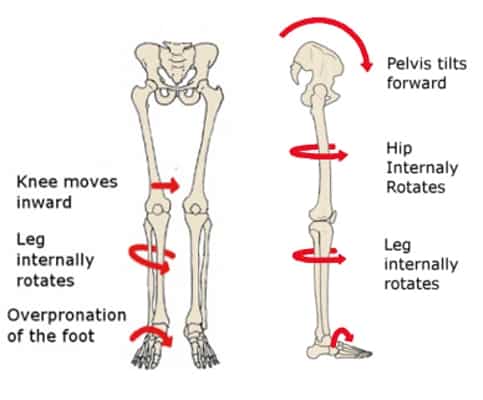
Internal rotation cascade
- Overpronated foot -> internally rotated tibia -> internally rotated femur (thigh bone) -> internally rotated hip
- Your entire leg spirals inward with each step
- The ball of your hip joint no longer sits properly in the socket
Glute shutdown
- Your glute muscles (especially gluteus medius) are supposed to stabilize your pelvis when you walk
- When your hip is internally rotated, these muscles can't fire properly; they get "inhibited"
- Weak, inhibited glutes can't control hip motion, so the problem gets worse
- This is called gluteal amnesia. Your glutes literally forget how to work
Compensation patterns develop
- Your hip flexors (front of hip) tighten to compensate for weak glutes
- Your TFL (tensor fasciae latae) and IT band work overtime
- Your piriformis (deep hip rotator) gets stressed and can pinch your sciatic nerve
- Your low back muscles strain to stabilize what your hips can't
The Trendelenburg Gait Pattern
When foot collapse leads to weak glutes, you often develop what's called a Trendelenburg gait. Your pelvis drops with each step, and your torso leans to compensate.
- Hip pain (especially on the outside or in the front)
- SI joint dysfunction (where your spine meets your pelvis)
- Low back pain
- Uneven wear on hip joints (leading to early arthritis)
Common Hip Conditions Linked to Foot Problems
- Hip osteoarthritis (accelerated joint degeneration)
- Greater trochanteric pain syndrome (lateral hip pain, often misdiagnosed as "bursitis")
- Hip impingement (FAI—femoroacetabular impingement)
- Piriformis syndrome (sciatica-like pain)
- Hip flexor tendinitis
- Labral tears (damage to the cartilage rim of the hip socket)
Research shows that people with abnormal foot mechanics have altered hip kinematics (movement patterns), and this increases the risk of hip pain and degeneration over time.
The Complete Kinetic Chain: How Everything Connects
Let me paint you the full picture of what happens when you walk with collapsed arches:
STEP 1: Foot Contact
- Your heel strikes the ground
- Your arch should absorb shock and provide stability
- Instead, it collapses inward
STEP 2: Ankle Collapse
- Your ankle rolls inward excessively
- Your Achilles tendon twists
- Your lower leg rotates internally
STEP 3: Knee Rotation
- Your tibia (shin bone) twists inward
- Your kneecap gets pulled off track
- Force concentrates on the inner knee
- IT band and outer structures get stressed
STEP 4: Femur Follows
- Your thigh bone (femur) rotates internally
- Your hip joint position changes
- The ball doesn't sit properly in the socket
STEP 5: Hip Compensation
- Your hip rotates inward
- Your glutes weaken and shut off
- Your hip flexors and TFL compensate
- Your piriformis strains
STEP 6: Pelvis Shifts
- Your pelvis tilts or rotates
- One side may elevate
- SI joints get stressed
- Foundation for your spine becomes unstable
STEP 7: Spine Reacts
- Your low back increases its curve (hyperlordosis)
- Muscles on one side work harder than the other
- Vertebrae shift and misalign
- Upper back and neck compensate
And this happens thousands of times per day, every single day.
No wonder your knee hurts. No wonder your hip is tight. Your body is fighting a losing battle against faulty mechanics at the foundation.
Why Treating Just the Knee or Hip Fails
Now you understand why so many treatments provide only temporary relief:
Physical therapy for the knee helps strengthen the muscles and may reduce pain temporarily, but if the foot is still pronating and forcing rotation with every step, the stress continues and pain returns.
Cortisone injections in the hip reduce inflammation, but don't change the mechanics causing the inflammation. The relief lasts weeks or months, then the problem comes back.
Hip replacement surgery might be necessary if the joint is severely damaged, but if the foot mechanics aren't addressed, the new hip will experience the same abnormal stresses—and you'll likely develop problems in the other hip or in your knees.
Knee arthroscopy to "clean up" a meniscus tear might help temporarily, but the forces that caused that tear are still present. The research is clear: meniscus tears are strongly associated with abnormal foot mechanics.
This is why we must treat the system, not just the symptom.
The Chiropractic Solution: Treating the Whole Chain
This is where comprehensive chiropractic care becomes essential. We don't just look at your knee or your hip in isolation—we evaluate and treat the entire kinetic chain from foot to spine.
What Complete Treatment Looks Like
1. Foot and Ankle Correction
- Custom orthotics to control pronation and support arches
- Chiropractic adjustments to restore proper foot and ankle mechanics
- Mobilization of stiff foot joints
2. Knee Realignment
- Adjustments to restore proper tibial rotation
- Patellar mobilization to improve tracking
- Soft tissue work on tight structures (IT band, hamstrings, quads)
3. Hip Restoration
- Adjustments to restore normal hip joint mechanics
- Glute activation and strengthening exercises
- Release work on tight hip flexors and piriformis
- Proprioceptive training to retrain movement patterns
4. Pelvic Stabilization
- SI joint adjustments
- Pelvic alignment correction
- Core strengthening focused on functional patterns
5. Spinal Support
- Full spine adjustments to address compensatory patterns
- Postural correction
- Ergonomic and lifestyle modifications
The key insight: We're not just treating your painful knee or hip. We're removing the cause of the problem and restoring normal mechanics throughout your entire body.
Your Knee and Hip Action Plan
If you're dealing with chronic knee or hip pain that won't go away, here's what you need to do:
STOP doing this:
- Treating only the painful area
- Assuming the problem is where the pain is
- Accepting that you "just have bad knees" or need to "live with it"
- Thinking surgery is your only option
START doing this:
- Get a complete biomechanical evaluation from foot to spine
- Have your gait analyzed and your arches assessed
- Address foot mechanics with custom orthotics
- Get regular chiropractic adjustments to restore proper joint mechanics
- Strengthen the entire chain, especially your glutes
- Give your body time to adapt to proper mechanics
What to expect: Most patients notice improvement within 4-6 weeks when we address the complete chain. But remember—your body developed these compensation patterns over months or years. Complete resolution takes time and consistency.
The good news? Unlike treating just the symptom, when we fix the foundation and restore proper mechanics, the results last.
The Bottom Line: Look Downstream to Fix Upstream Problems
Your knees and hips are suffering because of what's happening at your feet. They're caught in the middle, absorbing stress and compensating for faulty mechanics with every single step.
You can keep chasing the pain: treating the knee, injecting the hip, eventually replacing joints. Or you can fix the foundation and let your body function the way it was designed.
Before you consider surgery, before you accept that pain is just part of getting older, before you give up activities you love, check your foundation.
The solution to your knee and hip pain might be 12 inches below where it hurts.
KNEE & HIP PAIN EVALUATION SPECIAL
Suffering with chronic knee or hip pain that won't go away?
This month ONLY, for FREE, we're offering a comprehensive Arch Evaluation Package including:
- Digital foot scan
- Gait analysis
- Posture evaluation
- Custom orthotic consultation
Reply to this email, call, or text to take advantage!
Don't treat the symptom. Fix the system. Get your evaluation and finally get answers about why your knees and hips hurt AND learn what to do about it.
Scientific References:
Barton CJ, et al. (2010). Foot and ankle characteristics in patellofemoral pain syndrome: a case-control and reliability study. Journal of Orthopaedic & Sports Physical Therapy, 40(5), 286-296.Levinger P, et al. (2010). Foot posture in people with medial compartment knee osteoarthritis. Journal of Foot and Ankle Research, 3, 29.
Gross KD, et al. (2011). Association of flat feet with knee pain and cartilage damage in older adults. Arthritis Care & Research, 63(7), 937-944.
Neal BS, et al. (2014). Foot posture as a risk factor for lower limb overuse injury: a systematic review and meta-analysis. Journal of Foot and Ankle Research, 7, 55.
Reinking MF. (2016). Exercise-related leg pain in female collegiate athletes: the influence of intrinsic and extrinsic factors. American Journal of Sports Medicine, 44(4), 973-980.
Tateuchi H, et al. (2011). Dynamic hip joint stiffness in individuals with total hip arthroplasty: a case-control study. Gait & Posture, 34(1), 86-91.
Nunes GS, et al. (2013). Clinical and biomechanical features of foot and ankle related to patellofemoral pain syndrome. Physical Therapy in Sport, 14(3), 178-184.


MAP
© 2026 Mind Body Spine Chiropractic. All Rights Reserved. Accessibility Statement - Privacy Policy - Terms and Services - Sitemap
Powered by: 